An Interesting Internal Medicine Case Study
Ronnie is a one year old Bulldog cross. He was fit and healthy until he collapsed within minutes of vomiting a large amount of food and rubber bits on a Sunday evening. Earlier that day, Ronnie had been chewing on a football and the rubber bits were part of this football. He was rushed to the Southampton Vetsnow practice, where he was diagnosed with a haemo-abdomen. He was treated supportively with boluses of fluid and referred on the Monday to SCVS for further investigations.

On initial presentation, Ronnie was quiet and weak. He had slightly pale mucous membranes. He was tachycardic and tachypnoeic with marked cranial abdominal pain. After starting boluses of IV fluids, he had a rapid abdominal ultrasonography to assess for free fluid and collect a sample of fluid, which confirmed a haemo-abdomen.
Blood work confirmed non-regenerative anaemia, mild thrombocytopenia, with panhypoproteinaemia, most consistent with recent blood loss. Clotting times were performed. APTT was normal but PT was just above normal. CT scan revealed a large volume of peritoneal effusion. There was rupture of the left lateral liver lobe with a large sentinel clot between the left medial and left lateral liver lobes. The liver parenchyma was mottled. The pancreas had a tiger-stripe appearance, which was suspected to be due to pancreatic oedema or pancreatitis.
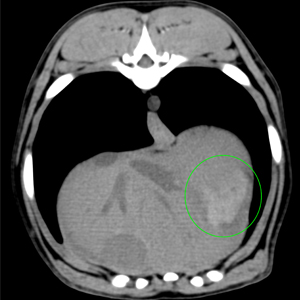
Pre contrast image showing blood clot (green ROI) between the liver medial and lateral left liver lobes
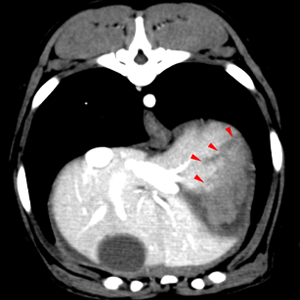
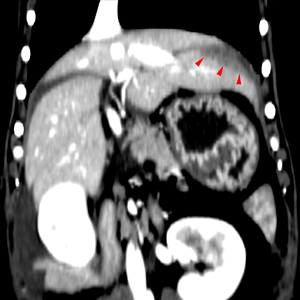
Post contrast images showing an irregular poorly contrast enhancing region (red arrowheads) within the cranial portion of the left lateral liver lobe. In order: transverse, sagittal, dorsal plane images.

Ronnie received a unit of fresh frozen plasma, while being prepped for emergency surgery to remove the ruptured liver lobe. Meanwhile we organised a blood donor (DEA 1.1 negative) to come in to collect a unit for Ronnie.
Midline laparotomy was performed. Following suction of the severe haemoperitoneum an active profuse haemorrhage was identified at the level of the left medial lung lobe. A pringle’s maneuver was performed. Briefly, a large Penrose drain was used to clamp temporarily the hepatoduodenal ligament (free border of the lesser omentum) interrupting the flow of blood through the hepatic artery and the portal vein and thus helping to control bleeding from the liver. When the haemorrhage was controlled, a thoraco-abdominal stapler was employed to perform a left medial liver lobectomy. The abdomen was then thoroughly lavaged and closed routinely.
At the end of surgery, PCV had dropped to 19%, blood pressure was low and Ronnie was tachycardic despite being on crystalloids, methadone, lidocaine CRI and dopamine CRI. The blood unit collected was administered. This raised the PCV to 34%. Ronnie became more stable although progressively jaundiced and regurgitating frequently. He was treated with metoclopramide CRI, omeprazole, lidocaine, opioids, maropitant and ondansetron and resumed eating and stopped regurgitating within a week.
Histopathology of the ruptured liver lobe was consistent with hepatic necrosis. Treatment with amoxicillin clavulanate and marbofloxacin was started at this stage (3 days post-surgery) as Ronnie had developed a marked band neutrophilia and pyrexia but also because of the known hepatic necrosis.
Ronnie was discharged from hospital 4 days later (7 days post-surgery) and is improving every day.
Spontaneous hepatic rupture is very rare.
In people, it is most often seen in association with pregnancy. The hypothesis is that vasospasm that results from increased sensitivity to circulating vasopressors and endothelial damage lead to formation of microthrombi, which cause hepatic necrosis, which subsequently lead to hepatic rupture. Other cases are most often associated with rupture of haemangiomas, primary or secondary malignancies, adenomas… Extremely rarely, spontaneous rupture with no underlying liver pathology has been described.
In dogs, there are very few reports in the literature. Sharpeis with amyloidosis and cats with amyloidosis are known to have an increase risk. We found two cases in the literature of spontaneous rupture and both had hepatic necrosis. One died and histopathology documented a Salmonella infection. This could however have happened post-mortem, as culture was obtained post-mortem. The other case survived to surgery and it was hypothesised that necrosis had been caused by mushroom toxicity but there was absolutely no evidence for this.
Our current case had no known exposure to any of the potential causes of acute hepatocellular necrosis in dogs (Amanita sp. mushroom poisoning, blue-green algae poisoning, idiosyncratic drug reactions to benzodiazepines, paracetamol, sulpha drugs, carprofen and amiodarone, ingestion of xylitol). Blunt trauma to the abdomen is possible but there was no report of it and no bruising on initial presentation. Unfortunately, the liver was not sent for culture so an infection of the liver could not be excluded but Ronnie only became pyrexic three days post-surgery so this is unlikely to have been the cause for the necrosis. Maybe Ronnie truly had spontaneous rupture of his liver and hypoxia resulting from acute haemorrhage caused the hepatic necrosis. We will most likely never know what truly happened but Ronnie’s liver function appears to be improving at this stage and he is likely to make a full recovery.
