Neurology case study – Spinal arachnoid diverticula
Raquel Trevail DVM, DipECVN, MRCVS. RCVS and European Specialist in Veterinary Neurology
A 2 year old French Bulldog was first presented to SCVS in December 2016. The owners reported that he was progressively getting weaker on pelvic limbs and there were a few episodes of urination and defecation while walking.
The neurological examination confirmed the weakness described by the owners. Palpation of the vertebral column was not resented but a vertebral malformation was suspected as kyphosis could be identified. The lesion was localised to the T3-L3 spinal cord segments and a congenital/ developmental problem such as arachnoid diverticulum and inflammatory disease were considered the most likely differential diagnoses.
MRI was performed and the findings were consistent with subaracnoid diverticulae at T9-T10 and secondary parenchymal changes in the spinal cord. The kyphosis was relatively mild and there were multiple other congenital spinal anomalies (transitional hemivertebrae and hemivertebra). A lumbar cerebrospinal fluid collection was performed and the results were within normal limits.
Louis recovered well and was discharged for monitoring. Surgical management was discussed at the time of discharge as further progression was likely to happen without it. Nevertheless possible surgical complications had to be considered.

In July 2017, Luis represented to us as gradual deterioration had been observed over seven months. Louis was still able to ambulate unassisted but there was certainly worsening of the weakness previously seen. A follow up MRI was discussed in view of pursuing surgical decompression.
MRI confirmed an increase in size of the diverticulum with also worsening of the intramedullary changes previously identified.
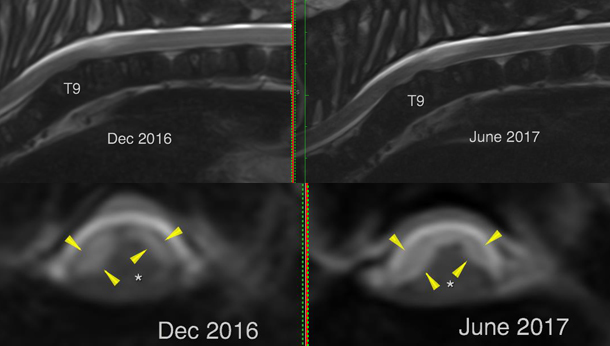
Sagittal and transverse T2w images acquired in December 2016 and June 2017 showing the increased size of the diverticula.
Surgery was undertaken and a dorsal approach to the thoracic vertebral column was made and T9 and T10 spinous processes were removed. A dorsal laminectomy was performed at this level and a cystic/ diverticulum was identified and a durectomy done. No surgical complications were seen at closure was routine.
Louis recovered well from the surgery but a few days later he was showing signs of deterioration. Dorsal compression secondary to seroma/haematoma was identified and surgery was once again undertaken. Louis significantly deteriorated and had to be hospitalised for four weeks. After a lot of rest and intensive physiotherapy Louis gradually regained he strength on his pelvic limbs and he is back on the paddle board.
Spinal arachnoid cysts are an uncommon cause of spinal cord compression. These cysts lack an epithelial membrane and therefore are not considered to be true cysts; they can be best described as intradural, extramedullary diverticula of the arachnoid. They result from an accumulation of cerebrospinal fluid (CSF) between two layers of the meninges and have several aetiologies. They are believed to be most commonly due to congenital/developmental abnormalities but they have also been described secondary to trauma, inflammatory disease or chronic compressive lesions such as intervertebral disc disease or vertebral malformations.
Pug dogs, French Bulldogs, and Rottweilers were the most commonly affected breeds reported in one study. Cervical lesions are seen most commonly in large breed dogs while thoracolumbar lesions are more common in small breed dogs. The most common cervical localization reported is C2-3 followed by C5-6, and in cases of thoracolumbar pathology, T13-L1 is the most commonly affected site. There is no age predisposition. Clinical signs can vary depending on the degree of compression and location within the spinal cord. Different degrees of ataxia and paresis can be seen with faecal, urinary incontinence, or both. The patients usually present with no signs of pain. Despite some wax and waning signs the disease is overall slowly progressive.
MRI, myelography or CT/ myelogram can be used for the diagnosis of spinal arachnoid diverticula. CSF analysis is usually undertaken in order to exclude an underlying inflammatory aetiology. Examination of CSF is usually within normal limits or may demonstrate nonspecific abnormalities, such as a mild elevation of nucleated cell count or protein content.
Treatment of choice consist of surgical management with durotomy or marsupialization of the dura matter. Like any other surgery, there are some risks associated with this procedures but the main concern is dorsal spinal cord compression secondary to inflammatory fluid or haematoma formation post operatively. Post-operative deterioration is not uncommon but is generally reversible. The aim of the surgery is to avoid further deterioration and hopefully in cases where the spinal cord is not compromise, to improve the presenting clinical signs. Non-surgical management is usually only undertaken in very young animals where the clinical signs are not too severe or in cases where the owners do not wish to proceed with decompressive surgery.